ShanghaiDoctor - Where China's Healing Wisdom Shapes Modern Medicine

Update time:2026-04-06Visits:3775
Profile
Dr. Xu Jin is Director of Pancreatic Surgery and a Doctoral Supervisor at Fudan University Shanghai Cancer Center. His academic journey began at Jianhu County Middle School in Jiangsu Province (1990-1993). In 1993, he was admitted to the prestigious seven-year clinical medicine program at the former Shanghai Medical University, graduating in 2000 with a master’s degree under the mentorship of Professor Ni Quanxing. He commenced his surgical career in the General Surgery Department of Huashan Hospital, later earning his doctorate in 2006 under Professor Ni’s continued guidance. In 2010, he joined the Shanghai Cancer Center, where he has served since.
With over two decades of expertise in pancreatic surgery, Dr. Xu specializes in diagnosing and treating a wide spectrum of benign and malignant pancreatic conditions. His distinguished research career includes four grants from the National Natural Science Foundation of China and the publication of more than 50 papers as first or corresponding author. His contributions have been recognized with numerous honors, including the Shanghai Municipal Health Commission Outstanding Young Medical Talent award, the First Prize for Outstanding Innovation Achievements by Shanghai Employees, and the Shanghai Excellent Invention Gold Award. He holds leadership roles as a Standing Committee Member of the Pancreatic Cancer Professional Committee of the Chinese Anti-Cancer Association and Chairman of the Neuroendocrine Tumor Professional Committee of the Shanghai Anti-Cancer Association.
A Surgeon’s Perspective
Time flows swiftly; the years pass like a melody. In memory, the days of childhood and student life retain a particular beauty and familiarity.
My centenarian grandfather, a practitioner of traditional Chinese medicine in our hometown, was the first beacon on my medical journey. I was fortunate that my path later led me to mentors like Professors Ni Quanxing, Fu Deliang, and Yu Xianjun. Following these guiding lights, I have navigated the vast ocean of medicine, striving to explore its depths with diligence and an unwavering pursuit of excellence. The seasons change without pause; what flows is time, but what endures is the essential quality and spirit passed down by my teachers. To me, this legacy holds a value more eternal than any material wealth—it is like being placed within a vast galaxy, looking up to see a constellation of wisdom shining brilliantly.
A healer, setting out with purpose, kindles the hope inherent in every life, enabling each patient’s personal universe to unleash its astonishing potential. I believe the trust between doctor and patient is paramount. A physician must convey an innate goodness, making the patient feel assured of a reliable ally. Only then, even in adversity, will a patient open their heart, cooperate fully with treatment, and together we can melt the ice of despair to create miracles of life. A true healer must invest heart, empathy, compassion, and professionalism to reap the most profound rewards.
Life’s path is seldom smooth, and the journey through pancreatic cancer treatment is especially fraught with challenge. Yet no matter the severity of the storm, a healer has a duty to help patients glimpse the dawn and forge a new beginning.
1. A Medical Heritage
Xu Jin was born here, and his connection to medicine traces back to his maternal grandfather, a local practitioner of traditional Chinese medicine. The elder was skilled not only in herbal remedies but also in performing minor surgical procedures for external injuries.
“Many people feel anxious at the mention of hospitals, but since childhood, I’ve felt a special closeness to them and to doctors. Scenes from those early years remain vivid: villagers would often sustain injuries while working the land, and serious wounds could easily become infected. Fortunately, my grandfather was highly experienced in treating such trauma, and the herbal medicines he used were remarkably effective. Growing up in that environment planted the earliest seed of a medical calling in me. By the time I filled out my university applications, I had developed a clear interest in medical fields.” Ultimately, with outstanding grades, Xu Jin was admitted to the former Shanghai Medical University’s combined bachelor’s and master’s program in clinical medicine.
Life in medical school was exceptionally full and intense—five years passed in the blink of an eye. During his master’s studies, Xu Jin met the most important mentor on his professional journey: Professor Ni Quanxing. “I was very fortunate; Professor Ni had a deeply reassuring presence. His diligence and rigor left a lasting impression on my medical career. I especially admired his simple, down-to-earth manner and quietly adopted it as my own ideal.”
Professor Ni’s influence on Xu Jin was so profound that to this day, Xu maintains the habit of making rounds every single day, weekends included. He feels something is amiss if he misses one. Xu Jin recalls, “Professor Ni was meticulous in everything. When reviewing our theses, his annotations were neat and color-coded, helping us move past vague understandings toward the essence of medical science. In clinical practice, he was even more thorough, dedicating himself wholeheartedly to his patients. What left the deepest impression happened years ago, when Shanghai’s public transport was far less developed. A patient from Taopu transferred multiple buses to reach the clinic, arriving covered in dust and with a long list of questions. Professor Ni answered each one in detail, pinpointed the key issues, and arranged the follow-up examinations to help the patient avoid unnecessary delays. In that moment, a bond of trust was instantly formed. He was like a respected family elder—kind yet authoritative. Everyone placed great hope in him, and I deeply admired that quality. To me, that is the very meaning of ‘the benevolent heart of a healer.’”
“There’s an old saying: ‘Surgery depends on operations, internal medicine depends on rounds.’ But with medical advances, our perspectives evolve. Rounds are crucial in both disciplines, though each doctor’s style may differ. Professor Ni’s approach was often relaxed, drawing from a wide range of references. Influenced by him, my own rounds aren’t overly formal. Sometimes I’ll hold a patient’s hand—pandemic permitting—or adjust their blanket, and ask about their needs and wishes. Occasionally I’ll even crack a joke or offer a light-hearted remark to lift their spirits.” Xu Jin believes that harmony between doctor and patient aids both treatment and recovery. “While on duty, I am their physician. But in daily life, we become friends—some patients even confide in me about family matters. Our conversations often extend beyond medicine; sometimes we help each other out.”
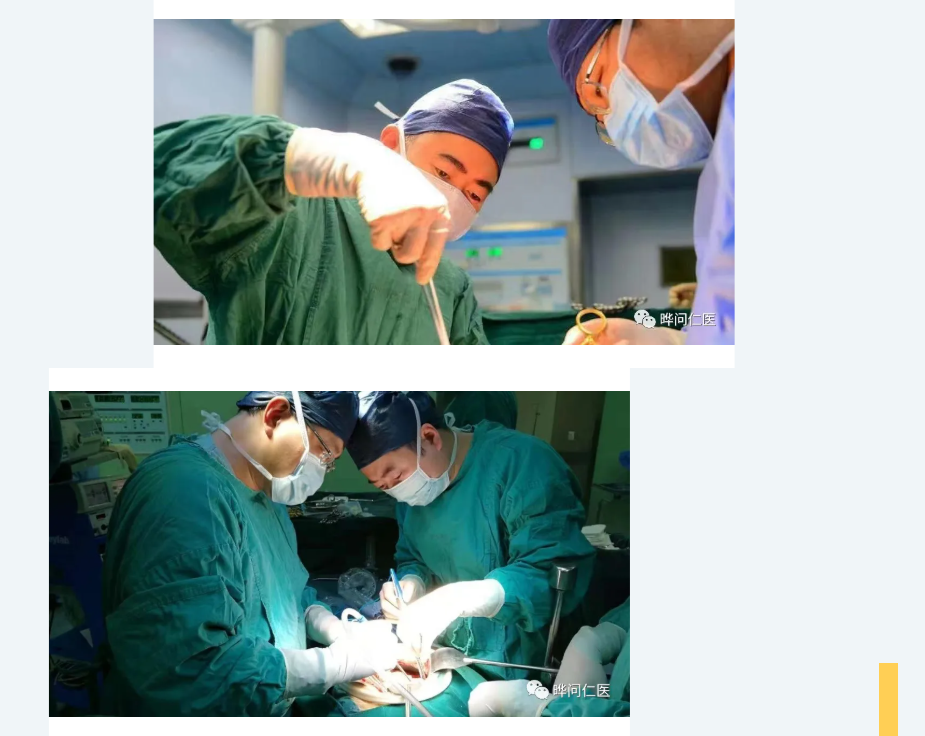
After decades in medicine, no matter how demanding his schedule, Xu Jin has maintained a routine: whenever he has a spare moment, he visits his surgical patients on the ward. On days he operates, he often rushes to check on them even before he has managed a few bites of food after leaving the operating theatre.
Between outpatient clinics, surgeries, departmental administration, and mentoring students, Xu Jin’s responsibilities seem endless. Colleagues and trainees frequently urge him to slow down. He always responds with a gentle smile: “Pancreatic surgery carries high risks, and a patient’s condition can be complex and change rapidly. Being an extra pair of eyes for them, taking that one extra look—that’s what gives me peace of mind.”
Today, many of Xu Jin’s patients and their families are eager to talk with him, to share their worries and hopes. Some patients, even after passing away, have left families who still keep in touch with him as they would a close friend. Xu Jin, in turn, treasures these rare, almost familial bonds. For him, the trust between doctor and patient is like a beacon, guiding those who are lost; it is also a safe harbour, offering calm and shelter to patients and families adrift in a sea of uncertainty.

2. The “King of Cancers”
Pancreatic cancer is often called the “king of cancers”—the most lethal, hardest to detect, and fastest-progressing of all major tumours. Among malignancies, it has one of the poorest prognoses, and many patients are already at an intermediate or advanced stage by the time they seek help.
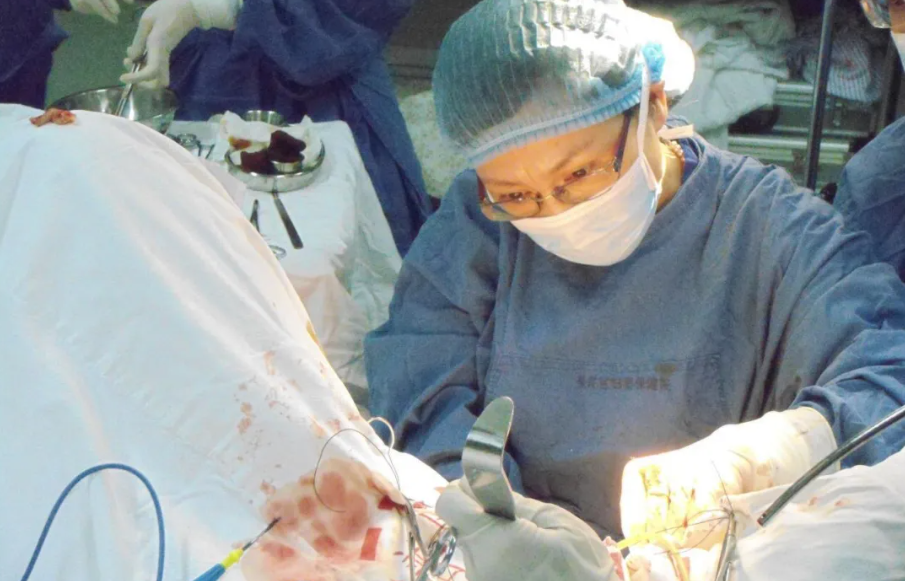
As one of the highest-risk and most technically demanding surgical specialties, pancreatic surgery is, as Xu Jin puts it with a wry smile, like dancing on the edge of a blade. “But as doctors, we cannot retreat. We must meet the challenge head-on. Our duty is to fight for every possible day of life for our patients.”
True to his word, in recent years Xu Jin has focused intensely on how to help pancreatic cancer patients live longer and better. With over twenty years of experience, he has pulled one patient after another back from despair, restoring hope and achieving what many once considered impossible.
Thanks to the efforts of Xu Jin and other leading pancreatic oncology specialists in China, the diagnosis and treatment of pancreatic cancer here have made significant leaps forward—even surpassing developed countries in certain areas. Speaking of these advances, Xu Jin’s pride is unmistakable.
“When I first specialised in pancreatic surgery, many doctors were still unfamiliar with the field. Over twenty years ago, when I arrived at Huashan Hospital, the department performed only about 20 pancreatic cancer operations a year. A major pancreatic procedure was still something of an event—colleagues would gather to observe. Now, we perform 2,000 pancreatic tumour surgeries annually, and treatments have become far more standardised, precise, and minimally invasive.”
Public awareness of the disease has also grown. Most people now recognise the severity of pancreatic cancer. Doctors are increasingly willing to offer public health education, and the public is eager to listen. This has helped create a social environment that encourages early detection and early treatment. In recent years, experts like Xu Jin have expanded community outreach, helping people understand the lifestyle factors and potential high risks associated with pancreatic cancer—empowering them to make changes that could reduce their risk from the outset.
With the earnest care of a teacher guiding a student, Xu Jin explains each step patiently and thoroughly. He speaks with a palpable urgency—not only anxious that the listener might miss a vital point, but deeply concerned that any patient under his care could overlook a crucial step in protecting themselves and their loved ones.
3. A Growing Light
In recent years, the arsenal of technological treatments for pancreatic cancer has expanded considerably, leading to marked improvements in both patient survival and surgical success rates. Over two decades ago, the overall five-year survival rate for pancreatic cancer stood at a mere 3%. Thanks to years of medical progress, that figure has now risen to 10%—a leap Xu Jin views as profoundly significant.
"Advances in surgical skill and instrument precision have greatly increased efficiency across many procedures," he explains. "Consider something as fundamental as the suture needle. We now use atraumatic needles, where the needle and thread are of uniform thickness. The thread follows the needle’s path exactly, minimising tissue damage. In the past, surgical needles resembled ordinary sewing needles, with a shaft thicker than the tip, which often caused bleeding when sutures were tightened. Furthermore, the development of minimally invasive techniques—laparoscopic and robotic surgery—alongside various other new technologies, works in tandem with traditional open surgery to enhance our effectiveness dramatically."
Xu Jin still recalls the longest pancreatic operation he ever performed, which began at 8:30 in the morning and did not conclude until 1:30 the following day. When it was over, he lay down directly on the operating room floor, completely spent.
"Today, a typical pancreatic cancer surgery takes about three hours. Even more complex cases rarely exceed five. In the past, we might schedule just one such operation per day, or even one every two days, and still find it exhausting. Now, we can comfortably perform two or three in a single day. This change is driven entirely by improvements in clinical technique and expertise."
The pharmacological landscape has also evolved. Xu Jin notes that over twenty years ago, when chemotherapy dominated treatment, response rates might have been as low as 5%. By 2010, drug efficacy had reached 15%, and today, certain single regimens can achieve response rates of up to 45%.
Survival rates for pancreatic cancer remain discouragingly low for many. Yet Xu Jin holds a firm belief: when doctors and patients build complete mutual trust and maintain thorough communication, physicians can help patients pursue the highest survival outcome possible. When doctors communicate with a patient’s family, if the patient places their full trust in the medical team, and the doctors commit wholly to the patient’s cause, the entire treatment process is greatly smoothed.
"This is why I believe our work with patients and their families must be meticulous," he says. "Patients and families should communicate openly with their doctors and genuinely strive for the best outcome. Doctors, in turn, must trust them. Then, no matter what difficulties or risks arise during treatment, everyone can stand together and fight. I believe every doctor is willing to give their all under such circumstances to achieve the best possible result."
For Xu Jin, the battle against pancreatic cancer—from treatment through recovery—depends on precision and comprehensive care at every single stage.
Xu Jin often says, "A doctor should never present a patient with a choice and leave it at that. Our role is to explain and clarify. A clear explanation is the most effective way to prevent doctor-patient conflict before it even begins. Patients are not experts. While they must be involved, the physician is best positioned to advise which treatment path is most suitable. We must clearly outline the pros and cons of every option, offer our constructive recommendation, and never abdicate that responsibility out of fear."
Having dedicated many years to pancreatic surgery, Xu Jin describes his work as tiring yet deeply fulfilling. "Once you choose to study medicine, you must commit to the profession—it’s a duty," he says, the weariness in his eyes giving way to clarity.
Every life moves forward along the course of its own history, gathering memories like branches and leaves along the way. Life’s existence is always tangible and vivid. Sometimes, all it takes is for the sunset to hand you a bundle of those branches, a single match, to let that gathered kindling lie quietly on the ground and catch flame. Even in the darkest night, you will see the fire, you will see hope. And when dawn returns, the lives of this world will once more find shelter under green boughs, vibrant and renewed.

ShanghaiDoctor.cn:
Professor Xu, pancreatic cancer is widely known as the "king of cancers." Are there identifiable high-risk factors in daily life linked to its development?
Xu Jin:
Yes, several high-risk factors are associated with pancreatic cancer. These include genetic susceptibility, family history, and certain lifestyle habits such as smoking, alcohol consumption—particularly heavy or chronic drinking—as well as diets high in sugar, frequent consumption of carbonated beverages, and obesity.
Additionally, some common conditions like diabetes have a relatively close relationship with pancreatic cancer. Acute and chronic pancreatitis are also significant risk factors.
Beyond these, there are potential occupational hazards, such as long-term exposure to certain chemicals, especially organic pesticides.
Furthermore, some benign tumors of the pancreas can carry a risk of malignant transformation. All these possibilities require careful evaluation by a specialist.
ShanghaiDoctor.cn:
Many pancreatic cancer patients also have diabetes. Why is the connection between the two so strong?
Xu Jin:
To understand this, we must look at the pancreas itself. It has two primary functions: exocrine and endocrine. The exocrine function, carried out by pancreatic acini and ducts, involves secreting digestive enzymes into the gut to break down food. Separately, scattered throughout the pancreas are clusters of endocrine cells called the islets of Langerhans. These release hormones, including insulin, directly into the bloodstream to regulate blood sugar.
Insulin is the body’s key blood-sugar-lowering hormone. As the name implies, it is secreted by the islets. When pancreatic cancer develops, it can damage islet function and impair insulin secretion, leading to elevated blood sugar and the onset of diabetes. Therefore, when a patient is newly diagnosed with diabetes, or an existing diabetic finds their blood sugar suddenly difficult to control, we must be alert to the possibility of pancreatic cancer. In such cases, diabetes may well be pancreatic cancer in disguise.
Pancreatic cancer can induce diabetes. Conversely, diabetes itself can promote the onset and progression of pancreatic cancer through various mechanisms. Their relationship presents a classic "chicken and egg" dilemma—it remains unclear which condition typically arises first. However, their frequent co-occurrence may offer valuable clues for the early detection of pancreatic cancer. Existing research indicates that pancreatic cancer can develop within three years following an abnormal rise in blood sugar levels.
ShanghaiDoctor.cn:
Can routine physical examination CT scans aid in the early detection of pancreatic cancer?
Xu Jin:
You are correct that pancreatic cancer is notoriously difficult to diagnose early. However, achieving early diagnosis is not necessarily as hard as it seems. The difficulty stems from the lack of specific early symptoms; the sensations are often similar to common gastrointestinal issues. Furthermore, routine abdominal check-ups primarily rely on ultrasound, which has significant limitations for examining the pancreas. Ultrasound is highly susceptible to interference from gas, and the pancreas is situated deep within the abdomen, obscured by the stomach and intestines—organs that contain air. This often makes it impossible to obtain a clear image of the pancreas.
In the last two to three years, we have actually seen an increase in early-stage pancreatic cancer diagnoses. This is largely attributable to the widespread use of chest CT scans during the COVID-19 pandemic. Previously, a routine chest X-ray was standard upon hospital admission. Now, many patients receive a chest CT. Although focused on the chest, this scan often captures the upper abdomen, including the pancreas. If an abnormal pancreatic shape is noted, an experienced radiologist will recommend further investigation. A subsequent thin-slice, contrast-enhanced pancreatic CT can then identify potential cases. Once a non-contrast CT suggests an abnormality, patients are advised to undergo this follow-up. Among those who do, approximately three to five in every hundred are diagnosed with pancreatic cancer—a significant detection rate.
This experience has provided us with practical insights. For individuals undergoing physical exams, we recommend including a few additional, inexpensive tumor markers, such as CA19-9 and CA125, for a minimal extra cost. Simultaneously, during a routine chest CT, the technician can be asked to extend the scan slightly downward to include the pancreas. Alternatively, during an abdominal ultrasound exam, a non-contrast abdominal CT scan could be considered (contrast-enhanced CT requires an injection and is not yet standard for routine screenings). If both these checks return negative results, it provides considerable reassurance.
ShanghaiDoctor.cn:
Is there a gap between China and developed countries like those in Europe and the United States in treating pancreatic cancer?
Xu Jin:
Our hospital has analysed survival rates for Stage I and Stage II pancreatic cancer patients. Previously, the three-year survival rate was only about 20%. Now, it has risen to over 40%, and the five-year survival rate has reached approximately 30%.
In the treatment of relatively advanced pancreatic cancer, significant breakthroughs have also been achieved. Last year, as part of our hospital’s 90th-anniversary review, we analysed survival rates among all malignant tumour patients treated here. The overall five-year survival rate for pancreatic cancer was approximately 10%—a figure essentially identical to the five-year survival rate reported in the United States in 2021, which also stood at 10%.
It is true that Europe and the United States have a greater number of clinical trials for new drugs, owing to their stronger pharmaceutical research and development capabilities. However, in terms of surgical technique, we have largely caught up with international standards. Therefore, in the overall management of pancreatic cancer, aside from being slightly behind in novel drug trials, our level of care is broadly comparable to—and in some respects even ahead of—that of other countries. In recent years, we have seen a number of patients return to China for treatment from abroad. This includes not only Europe and America; I currently have several patients who came back after receiving care in Japan. Having reviewed their treatment records from Japan, I found the approach to be almost identical to our own. Overall, I believe China’s standards are now largely in step with those abroad.
ShanghaiDoctor.cn:
What are the current treatment options for pancreatic cancer?
Xu Jin:
As with other solid malignant tumours, pancreatic cancer can be approached with a range of therapies. To date, surgical resection remains the only potentially curative treatment. However, because pancreatic cancer is difficult to detect early, only about 20% of patients are eligible for surgery at diagnosis. Many have already lost the opportunity for resection by the time the disease is identified.
That said, advances in surgical methods, chemotherapy and radiotherapy mean that some initially inoperable patients—including certain advanced cases with limited distant metastases, such as oligometastatic liver disease (with no more than three liver metastases)—can now become candidates for surgery after conversion therapy, significantly extending survival.
Chemotherapy is the most important adjuvant treatment alongside surgery. In particular, regimens such as Gemcitabine plus nab-paclitaxel and FOLFIRINOX have markedly improved outcomes compared with earlier options. Other approaches—including radiotherapy, targeted therapy, immunotherapy, traditional Chinese medicine and palliative local treatments—are also being progressively integrated. Together with surgery and chemotherapy, they form a comprehensive, multimodal strategy for pancreatic cancer.
Minimally invasive surgery is a shared goal for doctors and patients alike. However, because the pancreas is deeply situated and surrounded by major blood vessels, minimally invasive pancreatic surgery has developed more slowly than equivalent procedures in other abdominal areas.
Distal pancreatectomy, which requires no digestive tract reconstruction and involves fewer complex anastomoses, offers clear anatomical planes and faster recovery. It has become the preferred procedure for minimally invasive pancreatic surgery. Pancreaticoduodenectomy, by contrast, is far more challenging: it involves difficult resection, multiple anastomoses and considerable risk. For now, a minimally invasive approach for this operation is recommended only in select high-volume centres.
Furthermore, current minimally invasive techniques are used mainly for benign and low-grade malignant tumours. For highly aggressive pancreatic cancers—especially locally advanced cases involving major blood vessels—it remains unclear whether minimally invasive surgery is appropriate or offers clear oncological advantages. These questions will require further prospective clinical studies. Nevertheless, minimally invasive surgery is undoubtedly the way forward.
Editor / Chen Qing
If you need any help from Dr. Xu, please contact be free to contact us at Chenqing@ShanghaiDoctor.cn.
Dr. Gu Leyi | A 30-Year Odyssey of Healing, Innovation & Compassion
Dr. Lu Chunyan | Expert in Minimally Invasive Gynecologic Surgery and Pelvic Floor Reconstruction
Dr. Zhang Ti|Chasing Every Possible Chance Against Liver Cancer
Dr. Jun Li | Never Looking Back in Complex Hepatobiliary Surgery
Dr. Chen Jianghan | The Ones Most Deserving of Thanks Are my Patients
Dr. Huang Zheyong | Those That Outlast Life Itself in the Cardiac Realm
Dr. Wu Jiong | Treatment with Integrated Chinese and Western Medicine

Dr. Gu Leyi | A 30-Year Odyssey of Healing, Innovation & Compassion
Dr. Lu Chunyan | Expert in Minimally Invasive Gynecologic Surgery and Pelvic Floor Reconstruction

Dr. Chen Xu | From Challenging Early Service to Leading Minimally Invasive Gynecologic Care in Shanghai

Dr. Zhang Ti|Chasing Every Possible Chance Against Liver Cancer

Dr. Jun Li | Never Looking Back in Complex Hepatobiliary Surgery

Dr. Chen Jianghan | The Ones Most Deserving of Thanks Are my Patients

Dr. Jin Wei | Scaling the Heights of Anorectal Medicine

Dr. Huang Zheyong | Those That Outlast Life Itself in the Cardiac Realm

Dr. Shen Feng|The Endoscopic Life in the Digestive Tract

Dr. Wu Jiong | Treatment with Integrated Chinese and Western Medicine
Copyright © 2023 Yewen Renyi & ShanghaiDoctor.cn (This website is a non - profit medical humanities platform. The information contained herein is solely for biographical and historical purposes and does not constitute any medical advice.) 沪ICP备2023005392号-2 XML 沪公网安备31010902100835号
